Your Hand Hurts. Your Doctor Says Arthritis. But What If It’s Gout?
Picture this: a 58-year-old woman wakes up with a swollen, throbbing knuckle on her right hand. She cannot grip her coffee mug. The pain started overnight, and her finger looks red and angry. She goes to her doctor, who glances at it and says, “Probably osteoarthritis. You’re getting to that age.”
Sound familiar? It should, because this scenario plays out in clinics every single day. And too often, that woman actually has gout.
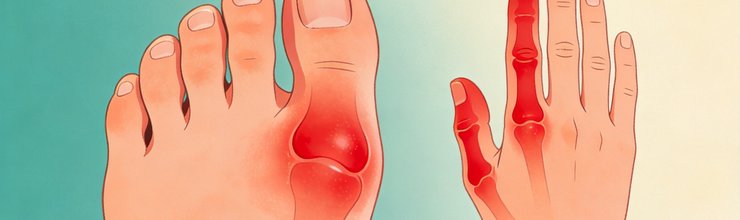
When you hear “gout,” you probably think of a man’s big toe turning red and purple after a steak-and-beer dinner. That image is so ingrained that even doctors default to it. But here is what the data shows: women with gout are far more likely to have their first flare in a hand, wrist, or knee. And because nobody expects gout in those joints, the diagnosis gets delayed for months or even years.
That delay is not just frustrating. It is dangerous.
The Big Toe Myth: Why Women Break the Classic Pattern
About 70 to 90 percent of men with gout have their first attack in the big toe. The reason comes down to temperature. Uric acid crystallizes more easily in cold environments, and your toes are the farthest joints from your body’s core. Lower temperature means lower solubility, which means crystals form faster.
But women’s bodies tell a different story. Research shows that women with gout frequently present with involvement in the upper extremities: fingers, wrists, and hand joints. Knees are also common. A review published by the American College of Rheumatology noted that gout in women “may affect the upper extremities first,” which is the opposite of what most clinicians expect.
A 2026 Moroccan cohort study comparing 92 men and 55 women with gout found that women were older at onset (average 64.9 years vs. 60.85 for men) and had significantly higher rates of hypertension and diabetes. While the monoarticular vs. polyarticular split was similar between sexes, women showed more renal involvement and less dramatic inflammatory markers. In plain terms: their gout looked different, quieter, and more systemic.
Why does this happen? Estrogen helps kidneys excrete uric acid. After menopause, estrogen drops, uric acid climbs, and crystals start depositing in joints throughout the body. But women also tend to have more comorbid conditions like osteoarthritis in their hands, which creates a perfect smokescreen. When a postmenopausal woman gets a swollen finger, both she and her doctor assume it is just wear-and-tear arthritis acting up.
If you want to understand why menopause flips the switch on uric acid, our deep dive on postmenopausal gout and estrogen breaks down the biology step by step.
When Gout Wears a Rheumatoid Arthritis Mask
Here is where things get really tricky. When gout shows up in multiple finger joints at once, it can look almost identical to rheumatoid arthritis (RA). Both conditions cause symmetric swelling, stiffness, and pain in the small joints of the hands. Both can produce nodules under the skin.
A case published in Rheumatology Advances in Practice (November 2025) drives this home. A 49-year-old woman arrived with symmetrical swelling in her metacarpophalangeal joints (the knuckles where your fingers meet your hand). Her doctors initially suspected seronegative rheumatoid arthritis, meaning her blood tests did not show the typical antibodies associated with RA. Blood tests for rheumatoid factor and anti-cyclic citrullinated peptide (anti-CCP) antibodies came back negative, which should have been a clue, but the clinical picture still pointed toward inflammatory arthritis.
The turning point? Visible tophi on her fingers and toes, plus a serum uric acid of 672 micromoles per liter. Her doctors stopped the diuretic she was taking, started allopurinol and colchicine, and within a month, her symptoms improved dramatically. Here is the kicker: she also had heart failure with an ejection fraction of 17 percent (a measure of how well the heart pumps blood, where 50 percent or higher is considered normal). After urate-lowering therapy, her cardiac function recovered to an ejection fraction of 54 percent. The gout diagnosis did not just save her joints. It may have helped save her heart.
This is not an isolated story. A separate case from the same journal described a 40-year-old premenopausal woman with intermittent joint pain in her ankles, wrists, knees, and shoulders. She was initially diagnosed with hypermobility syndrome. It took over a year and multiple flares before someone finally aspirated her ankle joint and found monosodium urate crystals. Gout confirmed.
These cases share a common thread: the diagnosis required someone to think outside the “gout equals big toe” box. For more on how women’s pain gets sidelined in clinical settings, read our analysis on why women’s gout pain gets dismissed.
Why a Delayed Diagnosis Hits Women Harder
Every month that gout goes untreated, uric acid crystals keep accumulating. They do not just sit there quietly. They erode cartilage, damage bone, and eventually form tophi, which are hard lumps of crystallized urate under the skin. Once tophi develop, joint damage becomes much harder to reverse.
A study from the UK, published in BMC Musculoskeletal Disorders, interviewed 14 women with gout about their diagnostic journeys. The findings were sobering. Many women experienced multiple flares over months or years before receiving a correct diagnosis. Several reported that their doctors did not even consider gout as a possibility because of their gender. One woman described feeling like “a freak of nature” because gout was supposed to be a man’s disease.
The consequences of delayed treatment go beyond joints. Women with gout tend to have more comorbidities than men: hypertension, diabetes, kidney disease, and cardiovascular problems. The Moroccan study found that women had significantly lower creatinine clearance (36.2 mL/min vs. 51.4 mL/min in men), meaning their kidneys were already struggling. Untreated hyperuricemia accelerates kidney damage and increases cardiovascular risk.
Our article on gout and joint damage from untreated hyperuricemia explains how silent crystal deposition works between flares, even when you feel fine.
The Osteoarthritis Trap
Osteoarthritis is the most common form of arthritis in women over 50. It causes bony enlargement in finger joints, stiffness, and aching. When a woman with osteoarthritis develops gout in the same joints, the symptoms blend together like watercolors on wet paper.
But there are telltale differences. Osteoarthritis pain builds gradually over years. Gout pain comes on fast, often overnight, with noticeable redness and warmth. Osteoarthritis produces hard, bony bumps (Heberden’s nodes). Gout can produce softer, sometimes chalky lumps (tophi) that are not attached to bone the same way.
The problem is that most primary care doctors see osteoarthritis every day and gout in women rarely. Confirmation bias kicks in: if it looks like osteoarthritis and the patient is a woman in her 60s, it must be osteoarthritis.
Some women also take diuretics for blood pressure, which raises uric acid. If you want to know whether your blood pressure medication could be feeding your gout, check our guide on diuretics and women’s gout.
How to Get the Right Diagnosis
If you are a woman experiencing sudden, painful joint swelling in your hands, wrists, or knees, here is what you should know about getting properly evaluated.
Ask for a serum uric acid test. This is a simple blood draw. Normal levels do not rule out gout (uric acid can drop during an acute flare), but elevated levels are a strong signal. If your doctor has not checked your uric acid and you have unexplained joint pain, request it directly.
Push for joint fluid analysis if possible. This is the gold standard. A needle extracts fluid from the swollen joint, and a microscope reveals the needle-shaped monosodium urate crystals. No other test provides definitive confirmation.
Ask about ultrasound. Dual-energy CT and ultrasound can detect urate crystal deposits in and around joints even without fluid aspiration. The “double contour sign” on ultrasound, a bright line over cartilage, is a hallmark of gout that does not appear in osteoarthritis or RA.
Track your flares. Keep a log of which joints hurt, when symptoms started, how long they lasted, and what you were doing or eating beforehand. This pattern data helps your doctor see the full picture instead of a single snapshot.
See a rheumatologist. Primary care doctors miss gout in women because they see it infrequently. A rheumatologist deals with crystal arthropathies regularly and is more likely to consider gout even when the presentation is atypical.
What Happens After Diagnosis
Once gout is confirmed, treatment follows the same principles regardless of which joint is affected. The goal is dual: stop the current flare and lower uric acid to prevent future attacks.
For acute flares, options include nonsteroidal anti-inflammatory drugs (NSAIDs), colchicine, or corticosteroids. The choice depends on your kidney function, cardiovascular health, and other medications. Women with hypertension or kidney issues may not tolerate NSAIDs well, so corticosteroid injections directly into the affected joint are sometimes the better route.
For long-term management, urate-lowering therapy with allopurinol or febuxostat brings serum uric acid below 6 mg/dL (360 micromoles per liter). If tophi are present, the target drops below 5 mg/dL (300 micromoles per liter). The medication starts low and increases gradually to avoid triggering flares during the adjustment period.
Here is something many women do not hear: stopping urate-lowering medication because you feel better is the most common reason gout comes back worse. Crystals dissolve slowly. It takes months of maintained low uric acid levels to clear deposits that have been building for years.
If you are in the early stages of understanding this condition, our guide to early warning signs of gout can help you recognize patterns before a full-blown flare hits.
The Bottom Line for Women
Gout does not follow the rules you were taught. It does not necessarily start in the big toe. It does not only affect men who drink beer. And it does not care whether your doctor expects to see it in your hands or knees.
If you are a woman with unexplained joint pain that comes on suddenly, involves redness and swelling, and affects your fingers, wrists, or knees, gout deserves a spot on the differential. The cost of missing it is not just prolonged pain. It is progressive joint damage, kidney strain, and cardiovascular risk that compounds with every untreated flare.
The good news? Once identified, gout is one of the most treatable forms of arthritis. The medications work. The targets are clear. The path forward is well-defined. You just need the right diagnosis first.
Frequently Asked Questions
Can gout start in your hand instead of your big toe?
Yes. While the big toe is the most common first site for men, women frequently have their first gout flare in finger joints, wrists, or knees. The American College of Rheumatology has noted that women may present with upper extremity involvement first. If you have sudden, painful swelling in a hand joint, ask your doctor to check your uric acid level.
How do doctors tell the difference between gout and osteoarthritis in the hands?
Speed of onset is the biggest clue. Osteoarthritis develops slowly over years with gradual stiffness. Gout attacks typically come on within hours, often overnight, with visible redness and warmth. Joint fluid analysis can definitively distinguish the two by identifying urate crystals under a microscope. Ultrasound looking for the “double contour sign” also helps.
Why is gout harder to diagnose in women than in men?
Three main reasons. First, gout is less common in women, so doctors think of it last. Second, women’s gout often appears in atypical joints (hands, knees, wrists) rather than the classic big toe, leading to assumptions of osteoarthritis or rheumatoid arthritis. Third, women’s flare presentations can be less dramatic with lower inflammatory markers, making the condition seem milder than it is.
Does gout in the knee mean the disease is more severe?
Not necessarily more severe, but it often means the disease has been present longer. Knee involvement tends to appear in people with higher uric acid burden or longer duration of untreated hyperuricemia. The larger joint space allows more crystal deposition before symptoms become obvious. This is why knee gout warrants a thorough workup including uric acid levels and imaging.
Should I see a rheumatologist if I suspect gout in my hands?
Yes, especially if your primary care doctor has not checked your uric acid or if your joint pain is not responding to standard osteoarthritis treatments. Rheumatologists are trained to distinguish between different types of inflammatory arthritis and have access to joint aspiration and advanced imaging. Early referral can shorten the diagnostic delay significantly.
References
- Singh JA, et al. “Why me? I don’t fit the mould… I am a freak of nature”: a qualitative study of women’s experience of gout. BMC Musculoskeletal Disorders. 2016. PMC4693432
- American College of Rheumatology. “Gout Beyond the Big Toe: Recognizing Uncommon Symptoms.” Patient Blog, February 2026. rheumatology.org
- El Kabli S, et al. “Sex-Related Differences in Gout: A Comparative Study in a Moroccan Cohort.” International Journal of Advanced Research. April 2026;14(04):18-22.
- Cooke H, Oke A. “Severe gouty arthropathy masquerading as inflammatory arthritis in a middle-aged woman with heart failure.” Rheumatology Advances in Practice. November 2025. doi:10.1093/rap/rkaf111.062
- Bahrani S, Sammut L. “Gout in a young premenopausal female: a diagnostic dilemma.” Rheumatology Advances in Practice. November 2025. doi:10.1093/rap/rkaf111.009
- Specialist orthopedic Centre. “Gout in Women: How It Presents Differently and Why It’s Often Missed.” December 2025. specialistortho.com.sg
- Neogi T, et al. 2015 Gout Classification Criteria: An American College of Rheumatology/EULAR Initiative. Annals of the Rheumatic Diseases. 2015;74(10):1783-1789.
Reviewed by the GoutSavvy Editorial Team